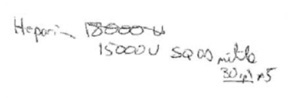
The following prescription for a patient who had been discharged from hospital was received by fax at a community pharmacy.
Would you dispense Heparin? Think again!
Medication mix-up with a faxed prescription
Heparin was dispensed, and the patient received two doses. When the hospital sent a request to the pharmacy to provide syringes and alcohol swabs for the duration of the “dalteparin” therapy, the community pharmacy recognized that an error had occurred.
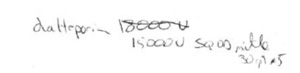
Further investigation revealed that the hospital had in fact sent a prescription for “dalteparin 15 000 U” (see below), but during fax transmission, the first two letters of the drug name, “da”. were cut off. The hospital’s fax transmission log indicated that the fax had been sent correctly, giving no indication of any problem.
This example was taken from the ISMP Canada Safety Bulletin, Vol. 12, No. 6, June 5, 2012. It is only one of many such scenarios ISMP receives.
What can you do to help minimize transmission errors when prescriptions are faxed?
- Educate all users about potential errors that can occur with faxes, scanners, and other technology and how to identify such errors.1
- Review all transmitted prescriptions for quality issues (e.g., truncation of a prescription header, extraneous marks in the prescription area), in addition to legibility of the prescription itself.2 In this case, the names of the prescriber and of the hospital, which appeared in the upper left-hand corner of the original prescription, were cut off during receipt of the faxed prescription.
- When faxing, ensure the presence of suitable margins, and avoid writing in the margin or borders of prescriptions.3
- Whenever possible, include both the generic and brand names of the intended medication, to provide an additional opportunity for verification. For example, integrate this information into computerized prescribing systems.
Refer to Ensuring Safe & Efficient Communication of Medication Prescriptions in Community and Ambulatory Settings for more tips.
References
- Improving medication safety in community pharmacy: assessing risk and opportunities for change. Horsham (PA): Institute for Safe Medication Practices; 2009.
- Fax machine “noise” = medication errors in waiting. ISMP Med Saf Alert. 1996 [cited 2012 May 22];1(13):1. Available from: http://www.ismp.org/newsletters/acutecare/articles/19960703.asp
-
ISMP quarterly action agenda — October–December 2004. ISMP Med Saf Alert. 2005 [cited 2012 May 22];10(2):3. Available from: http://www.ismp.org/newsletters/acutecare/articles/a1q05action.asp


