
Each practice incident and close call provides an opportunity for learning and implementation of changes to prevent recurrence.

To understand what went wrong, the pharmacy team must analyze the event to identify the contributing factors and root causes of the practice incident or close call. This process allows the pharmacy team to move beyond what happened, and to focus on why it happened. There are no right or wrong answers – it is simply important that the team think critically about the potential contributors to the practice incident or close call.
One of the most straightforward concepts that is employed in various methodologies is diagramming. Diagramming involves asking “why” to visualize the relationship between contributing factors and the outcome being analyzed, such as patient harm, or potential patient harm in the case of a close call.
Farida creates a cause-and-effect diagram to help the pharmacy team identify the various contributing factors to this practice incident.
She starts with the outcome: the patient experienced a hypoglycemic episode.
Then she identifies the practice incident that led to the outcome: the patient received rapid-acting insulin instead of long-acting insulin.
Then she works with the team to explore why this incident happened. Two conditions are identified: the incorrect product was selected, and the checking process was ineffective.
In evaluating why the incorrect product was selected, the team brainstorms potential contributing factors:
In evaluating why the checking process was ineffective, the team identifies several contributing factors:
Together, the team develops the following cause-and-effect diagram:
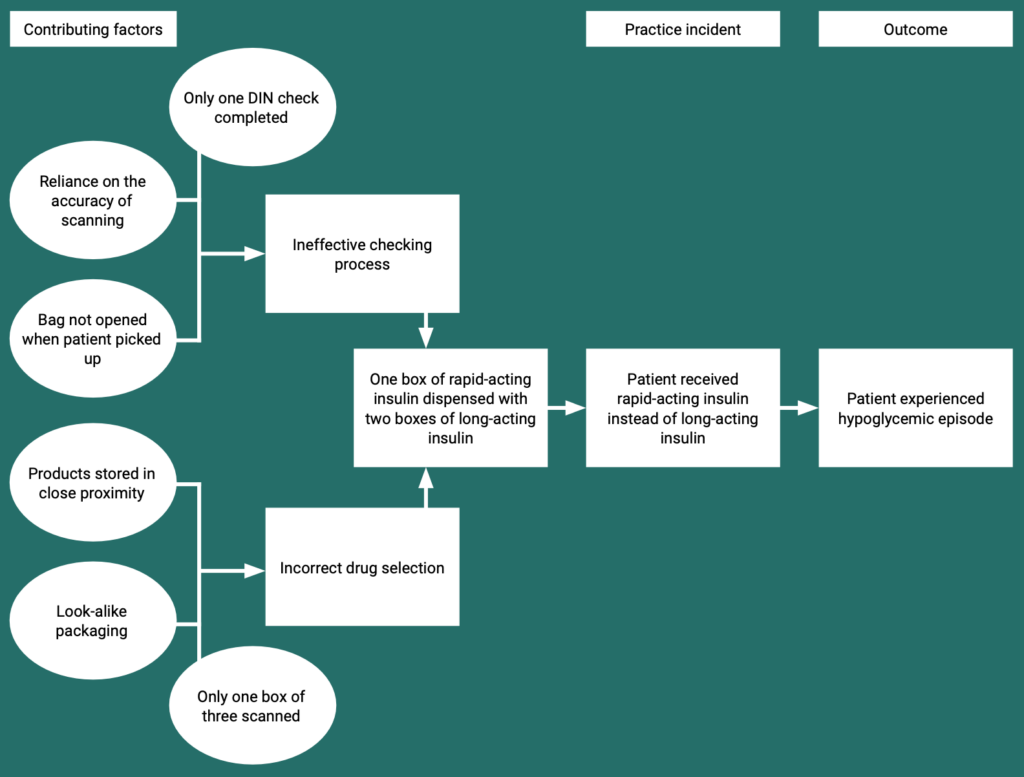
After reviewing the diagram together, the team agrees that look-alike packaging and storage of the drugs in close proximity are potential root causes, fundamental reasons this practice incident occurred.
Farida returns to her saved documentation in the pharmacy’s practice incident management platform to update the contributing factors. Her platform also allows her to upload a copy of the cause-and-effect diagram she created.
Farida selects the following contributing factors:
Several tools are available to support pharmacy teams in the exercise of identifying contributing factors and root causes (see the resources page), and various options will be included within the pharmacy’s practice incident management platform. Regardless of the tool(s) used, licensees must ensure that the process for analyzing practice incidents and close calls to determine contributing factors and root causes is clearly documented in the pharmacy’s policies and procedures.
The results of the pharmacy team’s analysis must be documented in the practice incident management platform and used to inform improvement activities.